

A
Anonymous would order again
A
Anonymous Great product
N
Nancy Strugar Great works made me tan :)


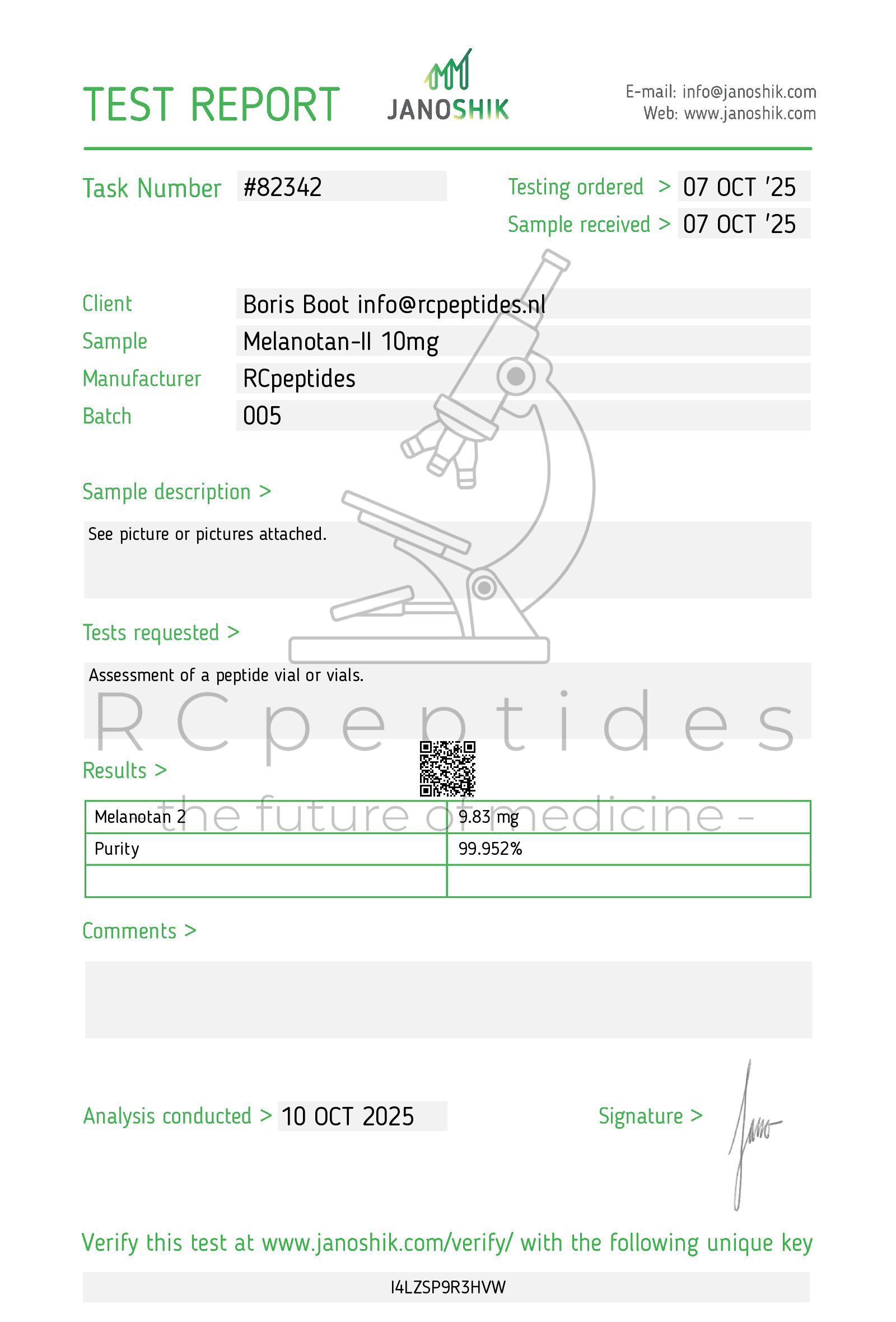
Melanotan-II 10mg vial
Pickup currently not available
NOT FOR HUMAN CONSUMPTION
Melanotan-II (MT-II) is a synthetic cyclic heptapeptide analog of the naturally occurring alpha-melanocyte-stimulating hormone (-MSH). It was originally developed as a tanning agent—stimulating melanin production to darken skin pigmentation—and has also been studied for its potential aphrodisiac and sexual function–enhancing effects.
Common Names: Melanotan-II, MT-2, MT-II
Chemical Classification: Synthetic peptide analog of -MSH (melanocortin receptor agonist)
Administration: Primarily subcutaneous injection, though nasal spray forms are sometimes sold (with questionable absorption)
MT-II binds to and activates melanocortin receptors (notably MC1R and MC4R). These receptors are involved in:
Melanogenesis (Skin Pigmentation)
MC1R activation in melanocytes increases the production of melanin, the pigment responsible for skin tanning and hair color.
Libido and Sexual Arousal
MC4R activation is implicated in sexual function and energy homeostasis. Some individuals report stronger libido and erections.
Appetite and Energy Regulation
Certain melanocortin receptors influence satiety and metabolism.
Tanning / Skin Pigmentation
Main Intended Effect: MT-II can increase melanin production, potentially providing a tanned appearance with less sun exposure and possibly some photoprotection against harmful UV rays.
Research Context: Initial research at the University of Arizona aimed to reduce the incidence of skin cancer by inducing tanning (protective melanin) without excessive UV exposure.
Sexual Enhancement
In both men and women, anecdotal and some clinical evidence suggest increased libido and arousal.
Erectile Function: MT-II has been studied in erectile dysfunction contexts and sometimes used off-label for this reason.
Appetite Suppression (Anecdotal)
Some users report decreased hunger, though this effect is variable.
Disclaimer: No standardized, FDA-approved dosing guidelines exist for Melanotan-II. The information below is derived from unregulated use, anecdotal reports, and limited research.
Subcutaneous Injection: Most commonly used route.
Typical “Starter” Dose: Ranges from 0.25 to 0.5 mg daily or every other day. Users often start low to gauge tolerance.
Maintenance Dose: Once desired skin tone is achieved, some individuals reduce frequency to 0.25–1 mg per week.
Loading Phase: Higher-frequency, small daily doses (0.25–0.5 mg) for 1–2 weeks until desired pigment is noticed, followed by a maintenance phase.
Individual Variation: Skin type, body weight, and general tolerance vary widely.
UV Exposure: Users typically still expose themselves to some UV (sunlight or tanning beds) to “activate” melanin production more effectively.
Over-Darkening or Hyperpigmentation: Excess use can cause uneven pigmentation or darkening of moles, freckles, and possible hyperpigmentation patches.
Nausea and Flushing: A characteristic “flushing” feeling and mild nausea often accompany doses, especially at higher amounts.
Appetite Changes: Appetite suppression (most common) or occasionally mild stomach discomfort.
Facial Flushing / Redness: Particularly shortly after administration.
Darkening of Moles and Freckles: Existing moles, freckles, and even new pigmented spots may appear or darken.
Uneven Tanning: Some users experience blotchy or uneven skin tone.
Spontaneous Erections / Enhanced Libido: Can be desirable or, in some contexts, inconvenient.
Melanoma Risk: Conflicting discussion on whether artificially increasing melanin could mask or potentially exacerbate underlying skin lesions.
Unknown Long-Term Effects: There is a lack of extensive, long-term human data on continuous MT-II use.
Cardiovascular or Metabolic Effects: Minimal data, but caution is advised given the melanocortin system’s role in metabolic regulation.
Pregnant / Nursing Women: Insufficient data, not recommended.
Pre-Existing Skin Cancers: Significant concern due to unknown impact on melanocytic neoplasms.
Serious Cardiovascular Conditions: Potential metabolic or blood pressure interactions.
Because Melanotan-II is unregulated in most countries:
Purity / Potency: Products sold online often lack third-party testing.
Contamination: Peptide powders may contain impurities, bacterial endotoxins, or other adulterants.
Safety Tip: Individuals seeking MT-II for any reason should verify product quality, review reputable sources, and consult a healthcare professional before use.
United States: Melanotan-II is not approved by the FDA for tanning or any medical usage. Often sold on the gray market or labeled “for research only.”
Europe & Other Regions: Similarly unapproved. Regulatory bodies issue health warnings about unlicensed usage.
WADA (Sports Doping): Not specifically listed as a banned substance, but athletes should confirm with updated doping guidelines and note possible doping test complications if used for performance enhancement of any kind.
Early, limited clinical research explored MT-II for sexual dysfunction (e.g., erectile dysfunction) and protective tanning.
Minimal large-scale, peer-reviewed, long-term studies exist due to regulatory and patent constraints, so safety and efficacy profiles are still not fully established.
Hadley ME, et al. (1998). Explored the tanning effects and potential for melanoma prevention.
Wessells H, et al. (2000). Studied the pro-erectile effects of MT-II in men with erectile dysfunction.
| Potential Benefits | Potential Risks / Drawbacks |
|---|---|
| Enhanced tanning with less UV exposure | Nausea, flushing, and potential adverse skin effects |
| Possible protective melanin boost | Unknown long-term melanoma risk |
| Increased libido / sexual arousal | Irregular pigmentation, moles / freckles darkening |
| Reduced appetite (anecdotal) | Unregulated product sources and purity concerns |
Melanotan-II can produce a tanned appearance and may enhance sexual desire, but unregulated use, unknown long-term risks, and possible adverse skin effects warrant caution.
Hadley ME, et al. (1998). “Melanotan II (MT-II): Effects on skin pigmentation and sexual function.” Annals of the New York Academy of Sciences.
Wessells H, et al. (2000). “Melanocortin receptor agonists, sexual function, and erectile dysfunction.” International Journal of Impotence Research.
Advance your research with our premium, high-purity research peptides and innovative laboratory compounds, crafted to deliver reliable results in the competitive scientific field. Buy research peptides from RCpeptides — your trusted peptide supplier dedicated to excellence in scientific research.
Chamber of Commerce number: 97286354
VAT number: NL005260308B91