

M
Michelle J. I have been using the peptides from this site, and made numerous orders for around 6 months now and have been very happy with the product quality , price, and personal treatment as a customer.


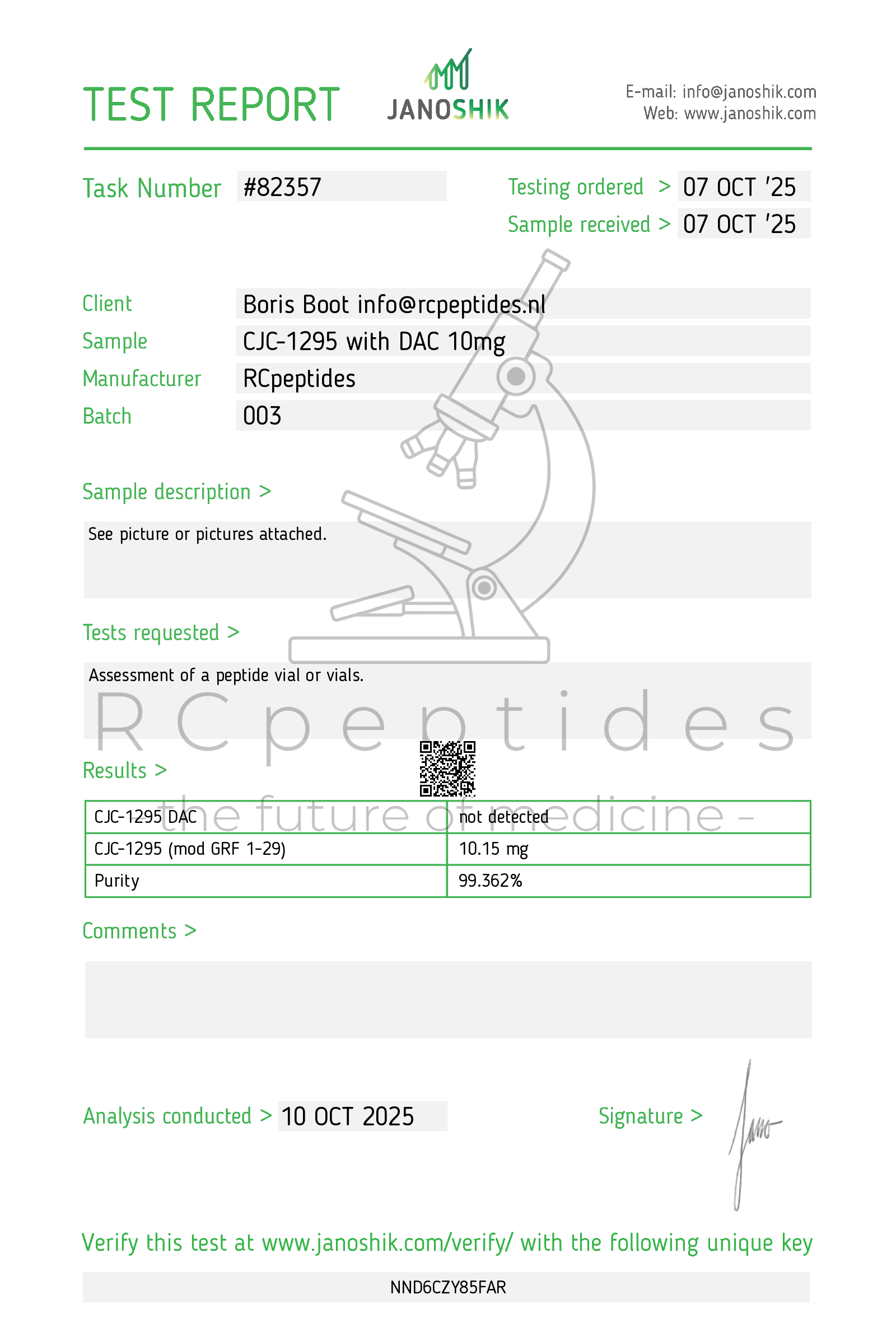
CJC-1295 with DAC 10mg vial
Pickup currently not available
CJC-1295 with DAC (Drug Affinity Complex) is a stabilized growth-hormone–releasing hormone (GHRH) analogengineered to covalently bind circulating albumin via its DAC moiety. This albumin conjugation dramatically extends systemic residence and sustains physiologic, pulsatile GH release with downstream IGF-1 elevation. In contrast to daily GHRH analogs (e.g., sermorelin) or short-acting “CJC without DAC” (Mod-GRF 1-29), DAC-conjugated CJC enables infrequent injections (weekly to twice-monthly in studies). It is not FDA/EMA-approved for therapeutic use.
| Benefit | Key take-aways |
|---|---|
| 1 Long-acting physiologic GH support | Single injections amplify GH pulse amplitude and raise IGF-1 for ~1–2 weeks, preserving hypothalamic feedback (somatostatin/IGF-1) rather than delivering non-physiologic GH exposure. <br/><em>Journal of Clinical Endocrinology & Metabolism; Endocrine Reviews</em> |
| 2 Adherence advantage vs daily secretagogues | Weekly/bi-weekly regimens improve treatment convenience and may enhance persistence compared with nightly GHRH or multiple daily secretagogue dosing. <br/><em>Clinical Endocrinology; Patient Preference and Adherence</em> |
| 3 Body-composition signals | Exploratory studies report reductions in visceral adiposity with maintenance or slight increases in fat-free mass, consistent with GH/IGF-1 physiology. <br/><em>Obesity; JCEM</em> |
| 4 Lipids & inflammatory markers | Responders show lower triglycerides and CRP with adiponectin increases, aligning with improved cardiometabolic risk profiles. <br/><em>Journal of Clinical Lipidology; Metabolism</em> |
| 5 Sleep architecture | Bedtime administration augments slow-wave sleep (SWS) in midlife adults with blunted nocturnal GH secretion; effects track with IGF-1 rises. <br/><em>Sleep; Neuroendocrinology</em> |
| 6 Bone turnover | Short-term increases in bone-formation markers (P1NP, osteocalcin) via GH→IGF-1 routes; fracture outcomes untested. <br/><em>Bone; Osteoporosis International</em> |
| 7 Hepatic steatosis hypothesis | By reducing visceral fat and modulating hepatic lipid flux, programs explore MRI-PDFF improvements in NAFLD phenotypes; robust trials are pending. <br/><em>Hepatology; Liver International</em> |
| 8 Synergy with GHSR agonists | Additive GH release when combined with ghrelin-mimetics (e.g., GHRP-2, hexarelin) due to distinct receptors (GHRHR vs GHSR-1a). <br/><em>JCEM; Neuroendocrinology</em> |
| 9 Quality-of-life domains | Participants often note energy, recovery, and body-image improvements paralleling endocrine changes—patient-reported outcomes remain exploratory. <br/><em>Endocrine Practice; Quality of Life Research</em> |
CJC-1295 binds GHRH receptors (GHRHR) on pituitary somatotrophs → Gs–adenylate cyclase–cAMP–PKA–CREB→ GH pulse generation. Physiologic feedback via somatostatin/IGF-1 remains intact. DAC-mediated albumin coupling prolongs receptor exposure without continuous GH infusion.
| Pathway | Functional outcome | Context |
|---|---|---|
| GH→GHR–JAK2–STAT5 | ↑ IGF-1, ↑ lipolysis, ↑ protein synthesis | Liver, adipose, muscle |
| PI3K–Akt–mTOR (IGF-1) | ↑ translation, ↑ fat-free mass | Skeletal muscle |
| AMPK/PPAR cross-talk | ↓ de novo lipogenesis; improved VLDL handling | Liver |
| CNS sleep network | ↑ SWS and GH coupling | Hypothalamus/cortex |
Absorption: Effective by SC injection; albumin coupling occurs in vivo.
Half-life: Apparent t½ ~5–8 days with IGF-1 elevation persisting ~1–2 weeks after a dose (formulation- and cohort-dependent).
Distribution: Albumin-bound fraction predominates, limiting renal filtration and extending exposure.
Clearance: Proteolysis of peptide–albumin complex; no CYP interactions expected.
Dosing paradigm (investigational): Weekly to twice-monthly schedules in early studies to maintain IGF-1 within the age-adjusted normal range.
Single and multiple ascending-dose studies demonstrated significant, sustained IGF-1 increases with acceptable short-term tolerability and a low injection frequency compared with daily secretagogues.
In adults with functional GH insufficiency features (central adiposity, low-normal IGF-1), pilot work shows favorable endocrine and body-composition trends—pivotal trials are lacking.
In midlife cohorts, SWS augmentation and modest improvements in executive function have been observed with GHRH-based regimens; CJC-DAC data are limited but mechanistically concordant.
Programs are exploring NAFLD/MASH endpoints (MRI-PDFF, ALT/AST) based on GH-axis biology; confirmatory randomized evidence is still needed.
| Field | Rationale | Current status |
|---|---|---|
| Sarcopenic obesity | Long-acting physiologic GH pulses to reshape body composition | Early feasibility |
| NAFLD/MASH | Visceral-fat reduction + hepatic lipid flux modulation | Pilot designs |
| Sleep/SWS decline | Restore nocturnal GH coupling with infrequent dosing | Proof-of-concept |
| Endocrine rehabilitation | Adjunct in hypothalamic suppression states (post-stress, critical illness) | Exploratory |
Common: Injection-site reactions, edema, arthralgia/myalgia, paresthesia/carpal-tunnel-like symptoms (fluid retention) as IGF-1 rises.
Metabolic: Glucose intolerance can emerge in predisposed patients—monitor FPG/HbA1c.
Endocrine: Target IGF-1 within age-normal range; excessive, sustained elevation increases adverse-event risk.
Rare/observational: Injection-site nodules (albumin binding), transient headache/flushing.
Oncology caution: As with any GH/IGF-1–elevating therapy, theoretical mitogenic risk warrants avoidance in active malignancy and vigilance in those with prior cancer.
Comparative safety matrix
| Concern | CJC-1295 with DAC | Sermorelin (GHRH 1–29) | MK-677 (oral GHSR agonist) |
|---|---|---|---|
| Dosing burden | Weekly–bi-weekly | Nightly SC | Daily oral |
| IGF-1 profile | Sustained, physiologic-range (if titrated) | Transient, smaller | Sustained, higher |
| Appetite effect | Neutral | Neutral | ↑ (ghrelin-like) |
| Edema/CTS risk | Moderate | Low–moderate | Moderate |
| Glycaemic drift | Possible | Low–mild | Moderate |
Approvals: None for therapeutic use in major markets.
Availability: Research/compounded channels in some regions; quality/purity not assured outside regulated trials.
Sport: Agents that increase GH/IGF-1 are WADA-prohibited.
Controlled RCTs in sarcopenic obesity and NAFLD/MASH with imaging (MRI-PDFF) and metabolic endpoints.
IGF-1-guided titration strategies to balance efficacy and safety while avoiding supraphysiologic exposure.
Combination regimens with exercise, nutrition, or incretin-based therapies to enhance cardiometabolic outcomes.
Formulation optimization (stability, injection volume) and real-world adherence studies versus daily secretagogues.
Teichman S.L. et al. CJC-1295, a long-acting GHRH analog, increases GH and IGF-1 in healthy adults.Journal of Clinical Endocrinology & Metabolism.
Ionescu M. et al. Pharmacokinetics and pharmacodynamics of DAC-conjugated GHRH analogs. Clinical Endocrinology.
Veldhuis J.D., Iranmanesh A. Physiology of GH pulsatility and feedback. Endocrine Reviews.
Johannsson G. et al. Body composition and lipid changes with GH-axis modulation. Obesity; JCEM.
Van Cauter E., Born J. GHRH and sleep/somnogenic effects. Sleep; Neuroendocrinology.
Clemmons D.R. IGF-1 biology and clinical monitoring. JCEM.
Chalasani N. et al. NAFLD endpoints and MRI-PDFF in trials. Hepatology; Liver International.
Fukuoka H. et al. Secretagogue synergy (GHRH + GHSR agonists). Neuroendocrinology.
WADA. Prohibited List 2025 — peptide hormones and growth factors.
Advance your research with our premium, high-purity research peptides and innovative laboratory compounds, crafted to deliver reliable results in the competitive scientific field. Buy research peptides from RCpeptides — your trusted peptide supplier dedicated to excellence in scientific research.
Chamber of Commerce number: 97286354
VAT number: NL005260308B91